She made history in 1978 as a member of the Milwaukee Does, playing in the first all-female professional basketball game against the Chicago Hustle in a new league called the Women’s Professional Basketball League (WBL). Forty-three years later, Gerry Lynn Booker’s trailblazing and pioneering spirit looks to digital dentistry to restore her smile and regain the confidence she once showed on and off the basketball court. When it came time to consider all the pros and cons of her restorative options, she and her clinician didn’t hesitate to choose a solution that was both definitive and aesthetic.
Introduction
Patients who present to the practice with terminal dentition due to advanced periodontal disease are challenging to treat. They are often anxious about losing their teeth and concerned about how the final prosthetic will impact their appearance. For the clinician difficult decisions must be made. Often not all teeth in the affected arch are terminal and could be considered worth evaluating and saving, especially if they offer functional advantages. However, efforts to save these teeth may present aesthetic challenges and the risk of patient displeasure with the final result. In addition, overarching considerations in the decision-making process must also be taken into account, including the patient’s financial situation, how treatment will benefit overall health or present adverse health risks in the future, and finally which treatment option will best address the patient’s stated goals.
For these patients conventional impression techniques also may present difficulties, especially if the teeth are mobile and/or painful. Aesthetic and blockout wax would be required with the risk of extracting teeth upon removal. Fortunately, advances in technology have provided clinicians with the tools to address many of these issues and offer the patient a preview of the highly aesthetic prosthetic that would result from treatment

Case Report
When Gerry Booker came to the practice, she had decided it was time to address the teeth in her upper arch (Figure 1). The mobility of her teeth was impacting her ability to chew and bite and their appearance made her very self-conscious (Figure 2). In our discussions she related that she was reluctant to smile, which had eroded her self-confidence in dealing with other people in her life including family and friends. Although she was nervous about losing her teeth, she was hopeful for a solution that would improve function as well as give her a natural-looking smile.

Evaluating periapical x-rays of her upper dentition (Figures 3) confirmed the unstable and mobile nature of the teeth in her upper arch. We discussed various restorative options. Each was explained in detail along with the benefits and risks as well as financial considerations and time in the chair to complete. She believed the immediate complete denture option best addressed her anxiety about tooth extraction and being able to leave the office afterward with a new smile. She also expressed a desire that the final prosthetic close the “gap” or diastema between teeth #8 and #9. However, she was still nervous about what the final prosthetic would look like before we proceeded to the next step.

One primary advantage of using digital technology is its immediacy in securing case acceptance. To help her feel more confident in the treatment proposal, we imported the preoperative digital photo we had taken of her existing smile into CAD smile design software (Trios Smile Design) and, as she watched, created a simulation of the proposed tooth shape, smile arc and design we believed would give her the natural-looking smile she desired. Upon viewing the result, she approved the treatment plan.
Due to the unstable nature of her maxillary dentition, it was decided a digital impression (Trios 4, 3Shape) would be the advisable approach for capturing the diagnostic impression of her maxillary arch (Figure 4). An intraoral scan would also allow capture of the soft tissue in static rather than compressive position and was now ready for digital design of the immediate denture.
Denture Fabrication
Critical to providing Gerry with the definitive solution she desired was the selection of the denture material and digital denture approach for creating her maxillary prosthetic. After careful consideration, we decided a monolithic prosthesis (Ivotion, Ivoclar Vivadent) would be the most efficient approach as well as provide her with the long-lasting strength and aesthetics she desired. The unique system combines high-quality tooth and denture base materials in a single bi-colour monolithic disc for creating natural life-like patient-specific aesthetics with the ability to shape and morph the denture teeth.



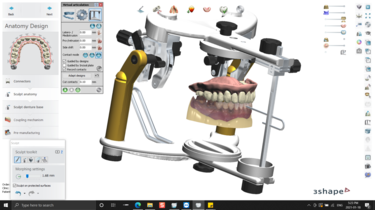
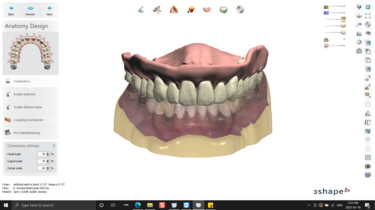
The intraoral impression scan was imported into the Ivotion 3Shape software where facially generated treatment planning principles were used to communicate and establish the tooth setup (Figure 6). Careful evaluation of the internal geometry of the Ivotion system ensured ideal tooth positions within the white portion of the monolithic disc and nicely demarcated and symmetric gingival contours within the pink section of the PMMA disc (Figures 7). The patient’s request to close the diastema between teeth #8 and #9 was accomplished as well as correcting the facially proclined incisors. A harmonious and consonant occlusal plane and idealized occlusion with her opposing arch were established (Figures 8 and 9).
Alvoeplasty surgery was planned on the day of delivery to provide a harmonious topography of the residual ridge. Precise alvoeplasty measurements were communicated to the laboratory for a 3D printed surgical guide that would aid in assuring sufficient alvoeplasty prior to delivery and soft relining of the immediate complete denture (Figure 10). The monolithic immediate complete denture was milled and delivered along with the surgical guide ahead of extraction and alvoeplasty surgery (Figures 11-14). After tooth extraction, alvoeplsaty surgery and a soft reline of the immediate maxillary denture were performed, restoring the patient’s function and desired aesthetics (Figures 15). After complete healing, a hard reline was planned for completion of a definitive removable solution.

Conclusion
Today, the ability to control all aspects of removable prosthetics from patient acceptance to final delivery through the use of digital technologies gives clinicians and technicians the tools needed to deliver a predictable, highly aesthetic prostheses with a workflow that is both efficient and precise.




